Running a home is not for the faint of heart. I have heard, seen, and in some cases tried to implement all manner of home productivity systems. Lately, our family has settled on a Skylight: the kitchen touchscreen where chores, the calendar, and the grocery list all live. It works, but it’s one of maybe six places household information actually lives. The school sends emails. Bills and shipping notices arrive in inboxes split between my wife and me. Appointments land on a Google Calendar. The mental work of pulling all of it together — what’s happening today, who’s doing which chore, which email actually needed a response — fell on a person. Mostly the person was my wife and that wasn’t what we wanted.
Synthesis is still hard. Figuring out next steps can be hard. I have been using LLM intelligence more and more in my life and was convinced that, with a little more synthesis, and a little more intelligence, I can reduce the load. I would have definitely bought this service if it existed. As far as I could tell, it did not. Claude Code had recently unlocked my ability to feasibly get back into coding, so I thought I would try to build it. My own Home Hub.
What it does
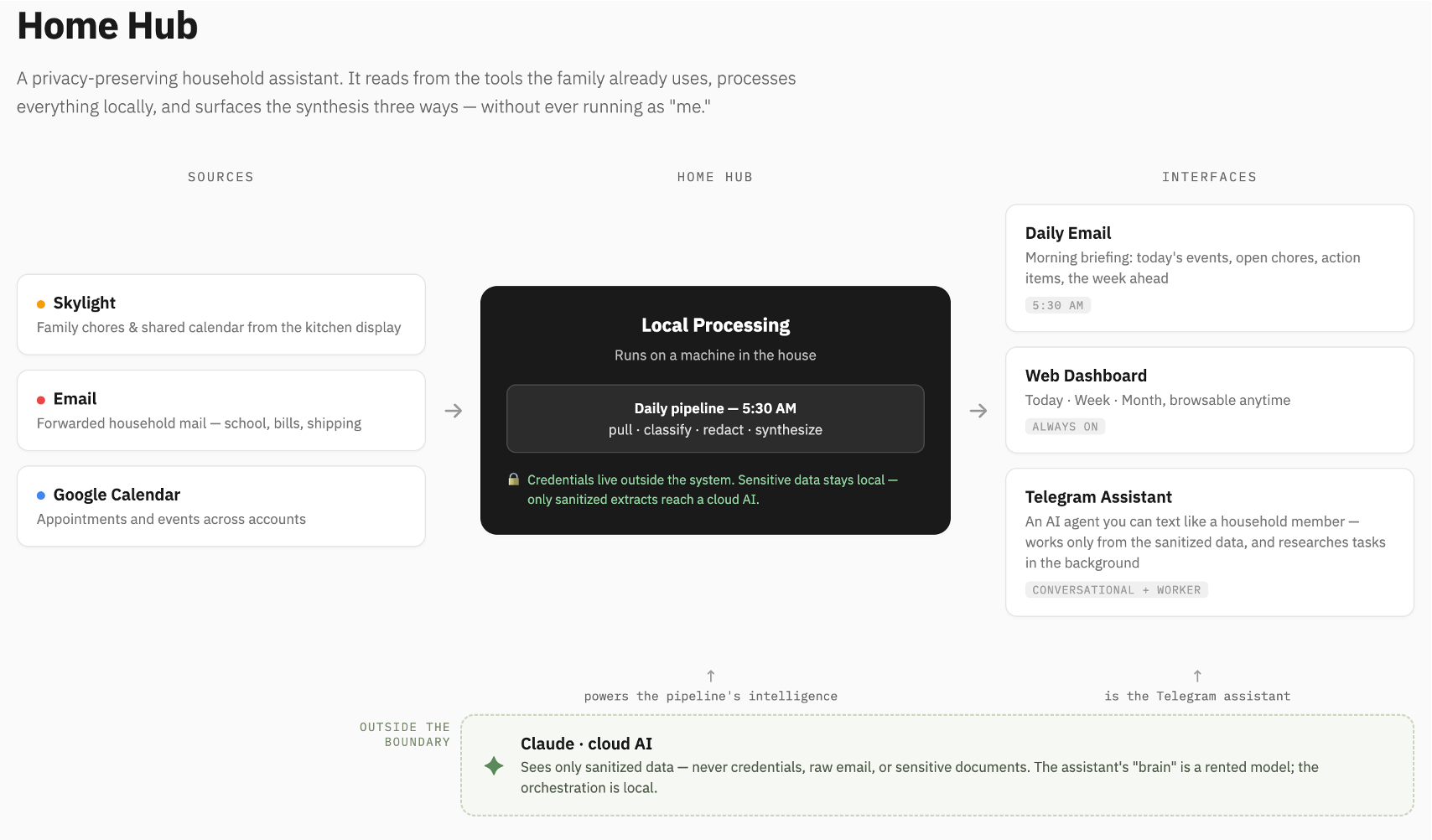
Home Hub is a privacy-preserving household assistant. It reads from the tools my family already uses — the Skylight (chores and the family calendar), a dedicated email inbox, Google Calendar — pulls everything into one place, and surfaces it three ways.
A daily email. Every morning at 5:30, before anyone’s awake, Home Hub assembles a briefing: today’s events, the open chores, the action items it found buried in overnight emails, and a look at what’s coming this week. It’s the synthesis that needed to come together in our heads, now done before breakfast.
A web dashboard. Includes prioritized views for today, this week, this month. The same information, browsable, when the email isn’t enough. It removes high-noise signals like repeating events so that we can, for example, focus on the bigger picture when a month’s view of Google Calendar otherwise just looks overwhelming.
An assistant you can talk to. This part has been the biggest unlock. Home Hub runs a conversational assistant over Telegram — I can text it like a member of the household. “What’s on for Saturday?” “Add a reminder to renew the registration.” It also works in the background: when there’s a task that needs research — compare three options, find a vendor, draft an email — it can take a first pass on its own and bring me something to review, rather than waiting to be asked.
The constraint that shaped everything
Here is the design decision I care most about: Home Hub does not run as me.
I was not interested in “connect all your accounts” tools that work by becoming you — full access, your login, your identity, acting on your behalf with the same powers you have. That’s convenient and, to my mind, the wrong model for something that touches my family’s email, calendar, and documents.
Home Hub works the way you’d want a trusted house-sitter to work. It has its own keys, scoped to what it needs, and you can take them back at any time without changing your own locks. Most processing happens in a sandbox, on a machine in my house. The genuinely sensitive material is airgapped elsewhere and separated out. Only sanitized extracts, stripped of the personal details, are ever handed to a cloud AI for the parts that need more horsepower.
But it’s the difference between an assistant I’d actually let near my family’s information and one I wouldn’t.
How it fits together
At the center is a small daily pipeline that does the unglamorous work: pull from each source, classify what’s sensitive, redact what needs redacting, and synthesize. Around it sit the three interfaces — the morning email, the dashboard, the conversational assistant — each reading from the same sanitized core.
(See the architecture diagram below.)
Why I could build this at all
It’s been a long time since I was building software regularly. Even then, small sections of this would have taken me a couple of weeks to implement. Five years ago, a project like this would have meant hiring someone, writing a requirements document, hoping the result resembled what I actually needed, and lots of iteration. The translation from what I know my household needs to working software was expensive enough that I simply would not have done it.
That translation cost has collapsed. With AI-assisted development, the person who understands the problem can increasingly build the solution directly — no intermediary, no requirements telephone game, no loss in translation. I know exactly what my family’s coordination problem looks like, because I live inside it. Now I can express that knowledge as a working system instead of as a feature request someone else might get wrong.
I think this is a small, domestic instance of a much larger shift we will see in our professional lives as well. For a long time, software was built by people who understood software, for people who understood the problem, with a lossy translation layer in between. As that layer thins, a shift will take place to people who understand the problem most deeply and are willing to build. In medicine, that’s the clinician who builds the tool instead of submitting a ticket. At home, that is me, usually while the kids are sleeping.
Home Hub isn’t really a product or package that I intend to share. I will probably get help from AI to consider that at some point. But for now it’s a household assistant that fits exactly one household — mine — because the person who built it is the person who needed it. That used to be a luxury reserved for good coders. I have proved, if only to myself, that it isn’t anymore.
 would add cost transparency to the complex, opaque medication supply chain believing that this will lead to lower prices and higher value care. Though this may appeal to our intuition, evidence that medication cost transparency leads to higher value care is scant. In order to add to the evidence base, four other investigators and I embarked on a 9-month investigation designing and evaluating the effect of medication cost transparency decision support built into the electronic health record. Bottom line: it makes a difference. The results were recently published and are available on the JAMIA website:
would add cost transparency to the complex, opaque medication supply chain believing that this will lead to lower prices and higher value care. Though this may appeal to our intuition, evidence that medication cost transparency leads to higher value care is scant. In order to add to the evidence base, four other investigators and I embarked on a 9-month investigation designing and evaluating the effect of medication cost transparency decision support built into the electronic health record. Bottom line: it makes a difference. The results were recently published and are available on the JAMIA website:  In aggregate, community health centers account for the care of about 20 million people in the US. Over half of these patients represent racial or ethnic minorities and over a fifth (22%) prefer to speak Spanish rather than English.
In aggregate, community health centers account for the care of about 20 million people in the US. Over half of these patients represent racial or ethnic minorities and over a fifth (22%) prefer to speak Spanish rather than English.
 The
The 
 Each year, half a million patients present to emergency departments in the US with acute vestibular syndrome (AVS) characterized by vertigo lasting more than 24 hours. Though this is frequently caused by something benign such as a self-limited viral infection, it may also indicate a more severe condition such as stroke of the posterior circulation. Unfortunately, MRI can miss strokes when obtained early in the disease course meaning half of those with with posterior strokes are inappropriately sent home from the ER.
Each year, half a million patients present to emergency departments in the US with acute vestibular syndrome (AVS) characterized by vertigo lasting more than 24 hours. Though this is frequently caused by something benign such as a self-limited viral infection, it may also indicate a more severe condition such as stroke of the posterior circulation. Unfortunately, MRI can miss strokes when obtained early in the disease course meaning half of those with with posterior strokes are inappropriately sent home from the ER. 
