Medication costs make up over 10% of health care dollars and are the fastest growing source of medical expense. Many state and federal officials have called for action that 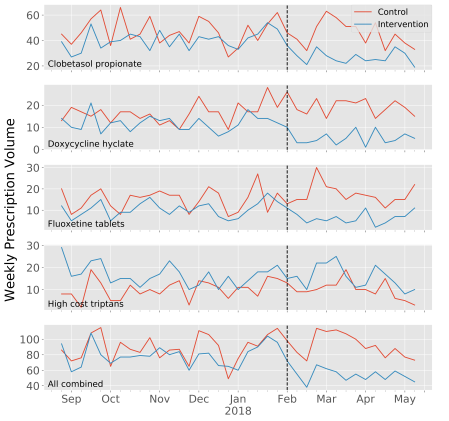 would add cost transparency to the complex, opaque medication supply chain believing that this will lead to lower prices and higher value care. Though this may appeal to our intuition, evidence that medication cost transparency leads to higher value care is scant. In order to add to the evidence base, four other investigators and I embarked on a 9-month investigation designing and evaluating the effect of medication cost transparency decision support built into the electronic health record. Bottom line: it makes a difference. The results were recently published and are available on the JAMIA website: https://academic.oup.com/jamia/advance-article-abstract/doi/10.1093/jamia/ocz025/5445905.
would add cost transparency to the complex, opaque medication supply chain believing that this will lead to lower prices and higher value care. Though this may appeal to our intuition, evidence that medication cost transparency leads to higher value care is scant. In order to add to the evidence base, four other investigators and I embarked on a 9-month investigation designing and evaluating the effect of medication cost transparency decision support built into the electronic health record. Bottom line: it makes a difference. The results were recently published and are available on the JAMIA website: https://academic.oup.com/jamia/advance-article-abstract/doi/10.1093/jamia/ocz025/5445905.
Objective
The purpose of this study was to determine if medication cost transparency alerts provided at time of prescribing led ambulatory prescribers to reduce their use of low-value medications.
Materials and Methods
Provider-level alerts were deployed to ambulatory practices of a single health system from February 2018 through April 2018. Practice sites included 58 primary care and 152 specialty care clinics totaling 1896 attending physicians, residents, and advanced practice nurses throughout western Washington. Prescribers in the randomly assigned intervention arm received a computerized alert whenever they ordered a medication among 4 high-cost medication classes. For each class, a lower cost, equally effective, and safe alternative was available. The primary outcome was the change in prescribing volume for each of the 4 selected medication classes during the 12-week intervention period relative to a prior 24-week baseline.
Results
A total of 15 456 prescriptions for high-cost medications were written during the baseline period including 7223 in the intervention arm and 8233 in the control arm. During the intervention period, a decrease in daily prescribing volume was noted for all high-cost medications including 33% for clobetasol propionate (p < .0001), 59% for doxycycline hyclate (p < .0001), 43% for fluoxetine tablets (p < .0001), and a non-significant 3% decrease for high-cost triptans (p = .65). Prescribing volume for the high-cost medications overall decreased by 32% (p < .0001).
Conclusion
Medication cost transparency alerts in an ambulatory setting lead to more cost-conscious prescribing. Future work is needed to predict which alerts will be most effective.
Author version of full article available here: Monsen et al Medication cost transparency JAMIA 2019
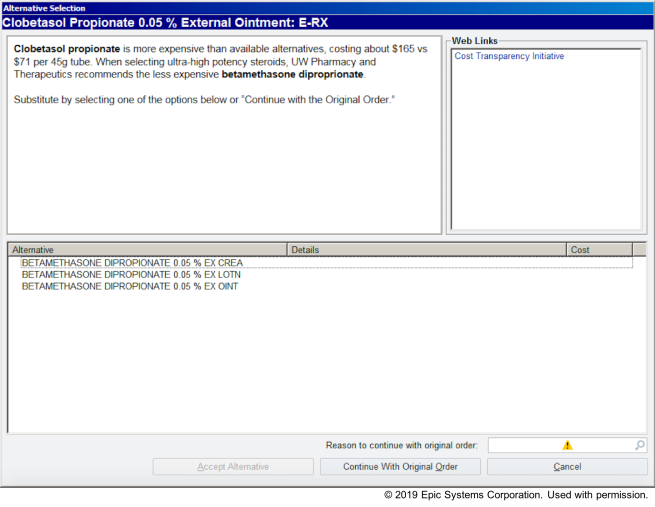
Decision Support Alert Implemented in EHR
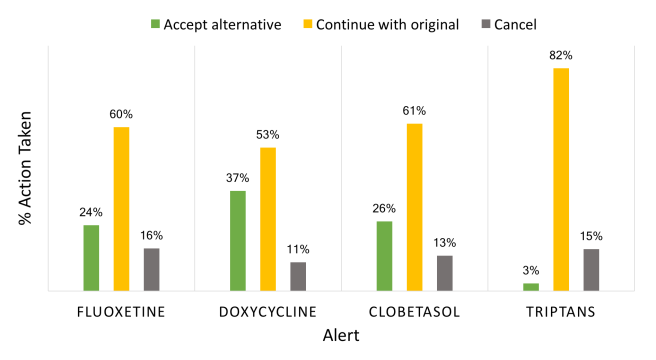
 Action Taken Following Alert Appearance
Action Taken Following Alert Appearance
Targeted High Cost Medications with Alternatives

