Medication costs make up over 10% of health care dollars and are the fastest growing source of medical expense. Many state and federal officials have called for action that 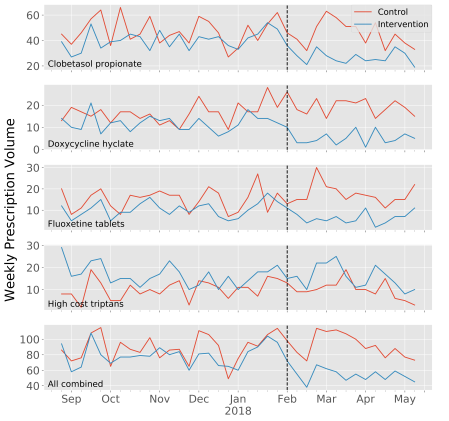 would add cost transparency to the complex, opaque medication supply chain believing that this will lead to lower prices and higher value care. Though this may appeal to our intuition, evidence that medication cost transparency leads to higher value care is scant. In order to add to the evidence base, four other investigators and I embarked on a 9-month investigation designing and evaluating the effect of medication cost transparency decision support built into the electronic health record. Bottom line: it makes a difference. The results were recently published and are available on the JAMIA website: https://academic.oup.com/jamia/advance-article-abstract/doi/10.1093/jamia/ocz025/5445905.
would add cost transparency to the complex, opaque medication supply chain believing that this will lead to lower prices and higher value care. Though this may appeal to our intuition, evidence that medication cost transparency leads to higher value care is scant. In order to add to the evidence base, four other investigators and I embarked on a 9-month investigation designing and evaluating the effect of medication cost transparency decision support built into the electronic health record. Bottom line: it makes a difference. The results were recently published and are available on the JAMIA website: https://academic.oup.com/jamia/advance-article-abstract/doi/10.1093/jamia/ocz025/5445905.
design
Problems and Promise of Medical Vocabularies
The Opinionated Electronic Medical Record
This post also appeared on KevinMD.
Software has opinions. No, I’m not talking about opinions on the next presidential election or opinions about flossing before or after brushing. Software has opinions about how data should be displayed, opinions about users’ comfort with the mouse, even, in some cases, opinions about what you should have for dinner (see your local on-demand food ordering service).
We tend to view software as a tool that is either good or bad. Good when it lets us do what we want with as little frustration as possible and bad when it doesn’t. Maybe we should be a little nicer to software.
Reach: Text-Message Appointment Reminder System
Problem
 In aggregate, community health centers account for the care of about 20 million people in the US. Over half of these patients represent racial or ethnic minorities and over a fifth (22%) prefer to speak Spanish rather than English.
In aggregate, community health centers account for the care of about 20 million people in the US. Over half of these patients represent racial or ethnic minorities and over a fifth (22%) prefer to speak Spanish rather than English.
Most CHC revenue comes from fee-for-service reimbursement paid by Medicaid (40%), private payers (7%), and Medicare (6%). This has led CHCs to pursue many of the strategies for maintaining solvency as other care centers across the US, including increasing patient visit volume and improving operational efficiency.
One problem all clinic sites face is the incidence of no-shows, patients for which an appointment is scheduled but that do not show up. It is estimated that no-shows account for 5-30% of appointments scheduled across the US and it is typically higher at CHCs. No-shows risk failing to deliver appropriate care to patients for whom they are scheduled in a timely or continuous manner, reduce access to scarce healthcare resources for those waiting for appointments, and represent up to 15% of lost revenue for the clinic.
Squire: Handheld Hospital Assistant

Problem
Effective hospital care requires coordination among multiple individuals including therapists, care coordinators, primary teams, consult teams, and nurses. Unfortunately, this coordination is costly to frontline staff often requiring much time and many steps even to identify the appropriate contact. Existing solutions have significant shortcomings without a highly-available best practice.
Killer Features of the Next Generation EMR
I was absent-mindedly playing with my iPhone today and took special notice of a feature I have rarely used before. If you swipe all the way to the left on the home screen, you will get a search bar to search all of your iPhone. This includes contacts, iMessages, and apps. I’ve never needed to use this before–a testament to the iPhone’s ease of use. Just prior to this, I was working on some patient notes using my hospital’s electronic medical record (EMR). In contrast, each task I performed required a highly-regimented, multi-click process to accomplish.
Criticizing EMR interfaces is a well-loved pastime among clinicians. Here, however, I am going to take an oblique approach and reflect instead on what has made good interfaces (all outside of medicine, it turns out) recognized as such.
Continue reading Killer Features of the Next Generation EMR on the THCB.
What Does the Massive Health Acquisition Really Mean?
If you’re like me, you’re extremely excited about the potential for design to reshape health care. I’m not talking health care system redesign (ACOs and such–though that’s great too), I’m talking about the type of design you see on Dribbble: the focus of a recent (awesome) HHS-sponsored competition.
One of the promising upstarts of health care re-design was a 2-year-old-or-so startup called Massive Health founded by ex-Mozillite Aza Raskin. Though I tend towards the skeptical, there was a part of me that thought that not only were they on to something, but they clearly had managed to aggregate real design talent. And in health care, no less! Apparently, I was not the only one as they convinced a number of investors to throw $2.25 million in to test out what they could do.
Continue reading What Does the Massive Health Acquisition Really Mean? on the Symcat blog.
