It’s been a while, partly because these posts still can take a while for me to write. I wanted to experiment putting a few thoughts down more informally (read: no links) and originally intended to elaborate on one of the often-overlooked problems with applying advanced statistical methods/ML/AI/”cognitive computing” to health care. That will have to wait though, because I’m realizing that there is some important background that I would like to elaborate on first. I’m going to preface this by admitting that I am no scholar on innovation, but I do consider myself a student. My thinking begins with a few practical (and very much borrowed) theories of innovation.
There are a lot of ways to think about the adoption and maturity of new technologies including Christensen’s “Disruptive Innovation”, Roger’s “Innovation Diffusion”, Kuhn’s “Scientific Revolutions”, or the hype cycle that has been popularized by Gartner. Maybe in another post I’ll talk more about those, but today I want to focus a little more closely on one that I have encountered mainly in the startup/Silicon Valley world: Perez’s “Technological Revolution”.
As far as I can tell, this is probably the closest to the Hype Cycle that has always seemed to resonate so well with health care IT folks. The theory describes a period of hype and capital investment during a so-called “installation phase” for a new technology followed by a more productive “deployment phase”. This image from the original work (via Chris Dixon’s blog) illustrates the concept:

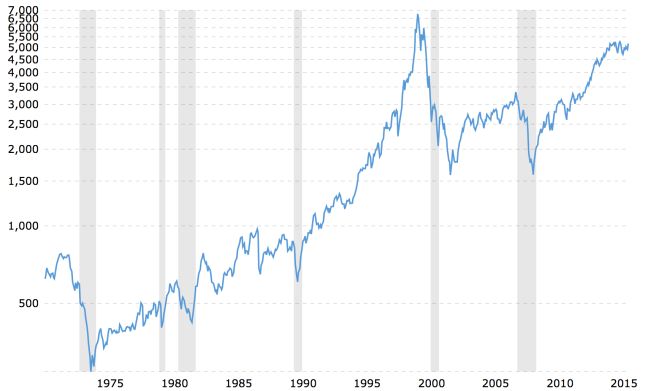
I suspect the model is attractive in Silicon Valley because it essentially describes the Dotcom era, market collapse, and gradual recovery that can be easily appreciated on casual inspection of the NASDAQ index from 1990-present:
I like the Technology Revolution model because it seems to fit the rapid uptake and installation that we have seen of electronic health records over the last decade or so and offers a little more rigor to why many people have been so disappointed with it. EHR adoption certainly began in earnest with a massive capital investment of public funds to the tune of $35B for Meaningful Use incentives plus private funding of many millions and sometimes billions for health care organizations to capitalize EHR roll outs. Unlike the NASDAQ, I don’t see health care organizations reneging–or whatever the health IT equivalent of shorting stocks is–on their multi-million dollar EHR investments, but the disappointment and desire for improvement is palpable.
To that point, I also like the Technology Revolution model because it is one of the answers to what has become known as the Information Technology “Productivity Paradox”, which is best summarized by Nobel Laureate Robert Solow’s quote: “we see computers everywhere except in the productivity statistics”. The question might be asked “why has health care remained fundamentally unchanged in terms of practice and productivity despite the availability of reliable computing for 60+ years?” Granted, there are assumptions behind that question that might easily be refuted if you focus on certain specialties or treatment modalities, but I think framing the question this way maintains a healthy amount of veracity if you spend a little time in a hospital or ambulatory practice or talking to a doc.
If you accept mine as a reasonable formulation of the Productivity Paradox, then the answer the Technology Revolution model might suggest is “well, we haven’t seen productivity gains yet because we are still in the installation phase.” You don’t need to dig very far into the health care clinic or IT departments to appreciate that we are very much still installing. If you are a physician, you have no doubt heard enough of “Big Bangs”, “Optimizations”, and “Change Management” to make you want to retire. Even some of my patients have commented to me “why don’t EHRs work better?”
You may prefer to think that much of health care IT transformation is just a “digitization” from a paper system. However, I am increasingly convinced that it is helpful to think about EHR adoption–instigated by Meaningful Use, quality incentives, and other forms of regulation–as a Technological Revolution. To the extent that this is true, then we can predict that in the trajectory of EHRs and their supportive technologies we will eventually enter the “deployment phase” expanding health care organizations’ capabilities while demanding changes in organizational structure, workflows, and jobs.
I don’t think these are earth shattering observations. While I hope this is interesting in its own right, all of this is really preface to a question I have been meaning to write about for a while (and what you are probably more interested in): why hasn’t “big data” really taken hold in the health care industry?
That’s for next time.
